|
| Guess What! - ESTP Case 5 |
The case is from a 20-week old male Wistar rat. The animal did not show any clinical, clinical chemical or ophthalmological abnormalities. Both eyes were normal at necropsy.
| Click on the images below for a larger view. |
|
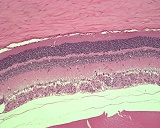
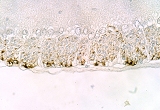
Fig. 1: H&E, x20
|
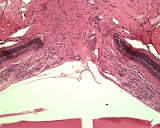
Fig. 2: H&E, x20
|
|
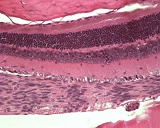
Fig. 3: H&E, x40
|
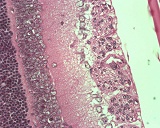
Fig. 4: H&E, x63
|
Morphologic Description
"Guess What"-Case no. 5 was characterized by a cellular thickening of the retinal opticus nerve fiber layer. The number of cells was substantially increased but the lesion was strictly limited to the opticus nerve fiber layer and did not distort other retinal layers. The cell nuclei were elongated and oriented in the direction of the opticus nerve fibers. They showed some tendency towards palisading. Cell borders were not recognizable. The cell nuclei were embedded in a meshwork of thin fibrils giving the appearance of a neuropil. When stained immunohistochemically for Glial Fibrillary Acidic Protein, the fibers reacted moderately positive (Fig. 5).
The optic nerves were not affected.
Proposed Diagnosis
Retinal Gliosis
Differential Diagnoses and Discussion
The glia-cell origin of the alteration was the most frequent answer. Retinal gliosis is an uncommon finding which usually occurs in aging rats (Yoshitomi 1990). This is not in accordance with our observation: In recent years, the finding was observed occasionally in animals aged 2 - 7 months.
Retinal gliosis has also been induced in certain experimental settings, e.g. by intraocular injection of nickel compounds (Albert et al. 1982) or by injection of autologous blood into the vitreus of rabbits (Kono et al. 1995).
By immunostaining for GFAP it has been demonstrated that the cells in question represent macroglial cells (Fig. 5). In the normal human retina, only astrocytes others than Mueller cells react positive for GFAP. However, Mueller cells may also express substantial amounts of GFAP, if they have been stimulated (Molnar et al. 1984). Therefore, the GFAP immunostaining cannot discriminate between astrocytes and Mueller cells, leaving the exact histogenesis of our proliferative lesion open.
We obtained some diagnoses suggesting a neoplasm: Malignant schwannoma or neurilemmoma, mixed meningioma, glioblastoma, and melanoma. Of course, the substantial increased number of glia cells gives the impression of a proliferative lesion, although it is strictly limited to the opticus nerve fiber layer and does not distort other retinal layers. However, due to the growth along predefined retinal structures it seems to be most likely that the proliferation is of reactive nature and is not preneoplastic or neoplastic.
Other diagnoses suggested were:
- Ectopic nerve bundles of the optic nerve
This seems to be unlikely, as the proliferation consists exclusively of glia cells and does not contain nerve fibers.
- Optic nerve dysplasia
It seems reasonable to call the lesion a dysplasia. However, due to its location in the retina, dysplasia of the optic nerve cannot be supported (the optic nerve was not affected).
- Extraocular orbital fibromatosis
This differential diagnosis can be excluded due to (I) the location and (II) the cellular composition of glia cells.
- One colleague suggested a congenital retinal malformation. This cannot be excluded, particularly when considering the relatively young age of the animals affected.
Other conditions leading to glia cell proliferation in the inner retinal layers are described for humans. Similar conditions may occur in rats and, therefore, have to be considered for differential diagnosis:
- An epiretinal membrane is a glia cell proliferation along the surface of the inner limiting membrane; it is caused by focal defects in the inner limiting membrane which allow glial cells to "break through" the retinal-vitreous interface; as glia cells get in contact with the vitreous body they are triggered to replicate and thus produce a thin veil of tissue.
- Massive retinal gliosis is described as a nonneoplastic proliferation of the retinal glia in response to diverse pathogenic states including trauma, congenital malformations, chronic inflammation, glaucoma, phtisis bulbi, and intraocular neoplasms (Yanoff et al. 1971). It is derived from Mueller cells (Nork et al. 1986) and appears as single or multiple well vascularized nodules.
- Massive preretinal proliferation is characterized by the outgrowth of retinal glia cells (astrocytes) through focal interruptions in the internal limiting membrane and, then, are located on the vitreous aspect of this membrane (Laqua 1975)
| Click on the image below for a larger view. |
|
Fig. 5: Inner aspect of the retina, including inner plexiform layer, opticus ganglion cell layer, and opticus nerve fiber layer, thickened by diffuse gliosis - GFAP immunostaining; note positive reaction of the gliosis; magnification: x40
|
References
- Albert DM, Gonder JR, Papale J, Craft JL, Dohlman HG, Reid MC, Sunderman FW Jr (1982) Induction of ocular neoplasms in Fischer rats by intraocular injection of nickel subsulfide. Invest Ophthalmol Vis Sci 22: 768-782
- Kono T, Kohno T, Inomata H (1995) Epiretinal membrane formation. Light and electron microscopic study in an experimental rabbit model. Arch Ophthalmol 113: 359-363
- Laqua H (1975) Massive periretinal proliferation (MPP) IV. Pre- and subretinal proliferation of glial tissue in experimental retinal detachment. Mod Probl Ophthalmol 15: 235-245
- Messmer EP, Ruggli GH, Apple DJ, Naumann GO (1997) Spezielle Pathologie der Retina. In: Naumann GO (ed) Pathologie des Auges. Second edition, Springer, Berlin Heidelberg New York pp 995-1152
- Molnar ML, Stefansson K, Marton LS, Tripathi RC, Molnar GK (1984) Distribution of S-100 protein and glial fibrillary acidic protein in normal and gliotic human retina. Exp Eye Res 38: 27-34
- Nork TM, Ghobrial MW, Peyman GA, Tso MO (1986) Massive retinal gliosis. A reactive proliferation of Muller cells. Arch Ophthalmol 104: 1383-1389
- Yanoff M, Zimmerman LE, Davis RL (1971) Massive gliosis of the retina. Int Ophthalmol Clin 11: 211-229
- Yoshitomi K, Boorman GA (1990) Eye and associated glands. In: Boorman GA, Eustis SL, Elwell MR, Montgomery CA Jr, MacKenzie WF (eds) Pathology of the Fischer Rat - Reference and atlas. Academic Press, San Diego pp 239-338
|
|