| Guess What! - ESTP Case 30 |
The lesion presented here was observed as an incidental finding in an approximately 4-month-old female transgenic mouse from a carcinogenicity study. The animal had a good nutritional status but had to be terminated due to sudden severe intestinal bleeding. No other clinical observations or gross lesions were reported.
| Click on the images below for a larger view. |
|
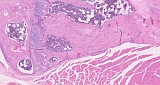
Fig. 1: H&E
|
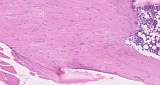
Fig. 2: H&E
|
|
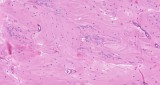
Fig. 3: H&E
|
Fig. 4: H&E
|
Morphologic Description
Case 30 shows a sample of the femorotibial joint with relatively long parts of the ossa femoris and tibia. The spicules of the metaphysis of the tibia appear to be slightly thicker and the diaphysis is somewhat bumpy and expresses a large area of mature osseous material in which no bone marrow cavity is visible (Figure 1). There is a connection to the growth plate via a broad spicule which is partly covered by a line of osteoblasts (Figure 2), however, the main lesion seems to be separated from the original bone growth from the growth plate. The newly formed woven bone shows a lamellar pattern resembling topographic contour maps with remnants of cartilaginous matrix (Figure 3). Only a few osteoblasts are found at the distal transition to the bone marrow cavity (Figure 4).
Proposed Diagnosis
Fracture (late stage of healing)
Differential Diagnoses and Discussion
Only three diagnoses were received for this case: Two of the participants suggested “increased bone” of the metaphyseal cortex arising from endosteum and periosteum. Increased bone is characterized by trabecular hypertrophy in the metaphysis which is seen either in the trabeculae (spongiosa) as expanded thickness or in the cortex, or in combination. This non-neoplastic augmentation of bone mass which has previously been referred to as hyperostosis or osteopetrosis, usually affects all bones is not restricted to just one location such as in the present case.
The third responder suspected an inherited abnormality rather than a sequel of a previous fracture due to the absence of callus. This cannot be excluded but we think that the presented case represented a late stage of fracture healing which might have occurred early in the course of the study (or even earlier).
Fractures of the tibia may occur incidentally due to handling, e.g. during shipment from the breeder or due to blood sampling procedures at the beginning of the study. Mostly, animals affected show severe lameness and are, in terms of animal welfare, removed from a toxicological study. Healed fractures therefore are an uncommon spontaneous finding in long-term studies in rodents. Most likely, this incidental finding would have been even missed, if the contralateral leg would have been taken for routine sampling.
Fracture repair consists of four overlapping processes: Inflammation, soft and hard callus formation and remodeling. Acute fractures of long bones are characterized by hemorrhage resulting in a hematoma, exudation of fibrin and eventually the presence of bone marrow cells. Pieces of broken bone may be also observed. This injury initiates an inflammatory response which is necessary for the healing process. Coagulation of the hematoma at the fracture ends and the bone marrow cavity is needed for the primary formation of the bridging callus. This early stage is followed by the production of external and internal calluses. For bone regeneration, specific mesenchymal stem cells have to be recruited which the proliferate and differentiate into osteogenic cells. Accordingly, external callus is formed by proliferation of fibroblastic mesenchymal cells (osteoprogenitors) in the periosteum proximal and distal to the fracture site. These progenitor cells migrate as a fibrin- and vasculature-rich granulation tissue to the fracture site along, where they differentiate and begin producing cartilage. This endochondral formation is key to the formation of cartilaginous callus, and in rats and mice this process has been shown to reach its peak 7 to 9 days post trauma. The primary soft cartilaginous callus then needs to be resorbed and replaced by a hard bony callus which is reached in rodents by approximately day 14 after injury.
Concurrent to the endochondral process, an intramembranous ossification response occurs in the subperiost of the proximal and distal ends of the fracture. This internal callus consists of woven bone in the medullary canal without passing first through the intermediate stage of cartilage formation.
Late stages of fracture healing are characterized by progressive remodeling and restoration of cortical and trabecular bone structure and is carried out by a balance of hard callus resorption by osteoclasts, and lamellar bone deposition by osteoblasts. Remodeling starts as early as 3 to 4 weeks but may take months or even years to be completed. Ideally, the external callus is gradually replaced by a lamellar bone structure, whereas the internal callus remodeling re-establishes a medullar cavity characteristic of a diaphyseal bone. This status has not been reached in the present case, in which a bone marrow cavity is not visible.
Although not an INHAND term or a discrete disease, reactive new bone formation would be probably another useful term for the lesion presented here.
Differential diagnosis may be osteoma that preferentially arises from the periosteal surface of the cortical bone. This benign neoplasm of osteocytic or osteoblastic origin shows a sharp demarcation of the surrounding tissue and is composed of very dense almost solid bone. It consists of irregular lobules of well-differentiated bone separated by narrow bands of fibrous connective tissue shows a disorganized arrangement of lacunae in the woven bone in contrast to the regular laminated architecture of the cortical bone. While in mice osteoma consists mainly of woven bone, rats show predominately a lamellar structure with only few cells. Spontaneous osteoma is rare in most strains of mice (only four cases in CD1 mice and in one male NMRI and one female C57bl mouse are recorded in the RITA Database among approximately 11.400 animals). They seem to be more common in females than in males (4:2) and most often occur in the skull. Osteoma is also rare in rats with 4 cases in males and 2 cases in females among approximately 20.000 animals of Sprague Dawley and Wistar strains.
References
- Fossey S et al. (2016): Nonproliferative and Proliferative Lesions of the Rat and Mouse Skeletal Tissues (Bones, Joints, and Teeth). J Toxicol Pathol 29 (3 Suppl) 49S-103S, DOI: 10.1293/tox.29.3S-2
- Fossey SL, Vahle JL and Leininger, JR (2018): Bones, Joints, and Synovia. In Boorman’s Pathology of the Rat. Elsevier, 299 - 319
- Hoeger H, Gialamas J, Jelinek F (1994): Multiple osteomas in mice. Vet Pathol 31: 429–434
- Marsell R and Einhorn TA (2011): The biology of fracture healing. Injury 42: 551–555
|