|
| Guess What! - ESTP Case 15 |
Common marmoset (Callithrix jacchus), female, adult (~ 8 years old).
Clinical history of chronic weight loss and reduced body condition; euthanasia due to poor prognosis.
At necropsy both kidneys were enlarged and pale and showed a finely granulated surface.
| Click on the images below for a larger view. |
|
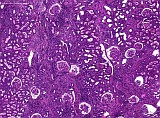
Fig. 1: H&E, x5
|
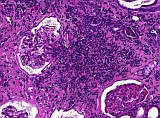
Fig. 2: H&E, x20
|
|
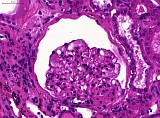
Fig. 3: H&E, x40
|
Morphologic Description
Case # 15 showed severe renal alterations including glomerular and tubulointerstitial lesions. In the glomerular tufts there was a diffuse, severe, segmental to global increase of PAS-positive mesangial matrix as well as distinct mesangial hypercellularity. Multifocally, dilation of Bowman's space, thickening of Bowman's capsule and adhesions of glomerular tufts with Bowman's capsule (synechiae) were observed. Findings within the tubular system included severe tubular atrophy, basement membrane thickening, tubular dilation and intratubular hyaline casts. These findings were accompanied by extensive interstitial mononuclear infiltration and severe multifocal interstitial fibrosis.
Proposed Diagnosis
Severe, diffuse mesangioproliferative glomerulonephritis (MPGN) with severe chronic tubulointerstial inflammation due to immune complex glomerulonephritis (ICGN); IgM/IgA-Nepropathy
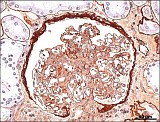
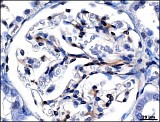
In comparable cases, methenamine silver staining on plastic-embedded semi-thin sections (~ 1 µm), immunohistochemistry (IgM, IgA) as well as transmission electron microscopy were performed. A mesangioproliferative character of glomerular lesions could be verified by silver staining (Fig. 4 ). Immunohistochemistry showed mesangial deposition of IgM and, to a lower degree, IgA (Figs. 5-6). Ultrastructurally, there were corresponding electron dense mesangial deposits within proliferated glomeruli (Fig. 7).
| Click on the images below for a larger view. |
|
Fig. 4: Movat's methenamine silver stain, x20
|
Fig. 5: IgM, x40
|
|
Fig. 6: IgA, x40
|
Fig. 7: TEM
|
Discussion
Twenty-eight contributions were received for this case:
Twelve contributors correctly suggested primary glomerulonephritis (GN) further characterized as membranoproliferative (2x), membranous (2x) or mesangial (1x) GN. There was no duplication of basement membranes as it is characteristic of membranous/membranoproliferative GN. Alterations were mainly restricted to the mesangium. Hence, the terms mesangial or mesangioproliferative are preferable.
Two contributors already suspected an immunopathogenic background in terms of IgG- or IgG/IgM-Nephropathy respectively. It could be shown that mesangial immune complex deposition in marmosets with MPGN is mostly consisting of IgM and IgA deposits.
The diagnosis chronic interstitial/tubulointerstitial nephritis was suggested by 8 contributors. The possibility of primary glomerulopathy was discussed by two contributors. One of them correctly underlined the necessity of immunohistochemical investigation to rule out immune complex deposition. Routinely performed evaluation of HE-stained sections does usually not allow differentiation between primary tubulointerstitial and glomerular alterations, especially in advanced cases like this one.
Further diagnoses included rather unspecific entities like chronic progressive nephropathy, nephrosis, familial/hereditary/juvenile renal disease and end stage renal disease. These diagnoses are not incorrect but miss a hint of an etiological background. To our knowledge, the term familial/hereditary/juvenile renal disease is normally used for a disease complex occurring in different breeds of dogs in early life with diverse pathogenic backgrounds.
One contributor suspected amyloid deposition. In comparable cases, detection of amyloid with Congo red stain is mostly negative. Moreover, there are usually no signs for primary bacterial infection, as it was suggested by another contributor.
MPGN is a common multifactorial disease pattern in marmosets. Immunohistochemical and ultrastructural investigations indicate an immunopathogenic background with predominant mesangial deposition of IgM and IgA. Therefore, the term IgM/IgA-Nephropathy of callitrichids has been proposed. The disease has a chronic progressive character usually leading to chronic renal failure in late life. It regularly occurs in association with the so called Wasting Marmoset Syndrome (WMS). Therefore, a positive correlation between WMS and ICGN is likely.
References
- Brack M, Rothe H (1981) Chronic tubulointerstitial nephritis and wasting disease in marmosets (Callithrix jacchus). Vet Pathol 18: 45-54
- Brack M, Schroeder C, Fooke M, Schlumberger W (1999) IgM/IgA nephropathy in callitrichids: Antigen studies. Nephron 82: 221-231
- Schroeder C, Brack M, Brandes F, Bruno SF (1997) Immune complex glomerulopathy in marmosets at the German Primate Center. Proc Am Assoc Zoo Vet 339-343
- Schroeder C, Osman AA, Roggenbuck D, Mothes T (1999) IgA-gliadin antibodies, IgA-containing circulating immune complexes, and IgA glomerular deposits in wasting marmoset syndrome. Nephrol Dial Transplant 14: 1875-1880
- Winkelmann J (2010) Nierenveränderungen bei Weißbüschelaffen (Callithrix jacchus) mit Wasting Marmoset Syndrom. Hannover, Tierärztliche Hochschule Hannover, Dissertation
|
|